WHO approves injectable lenacapavir in major shift on HIV prevention
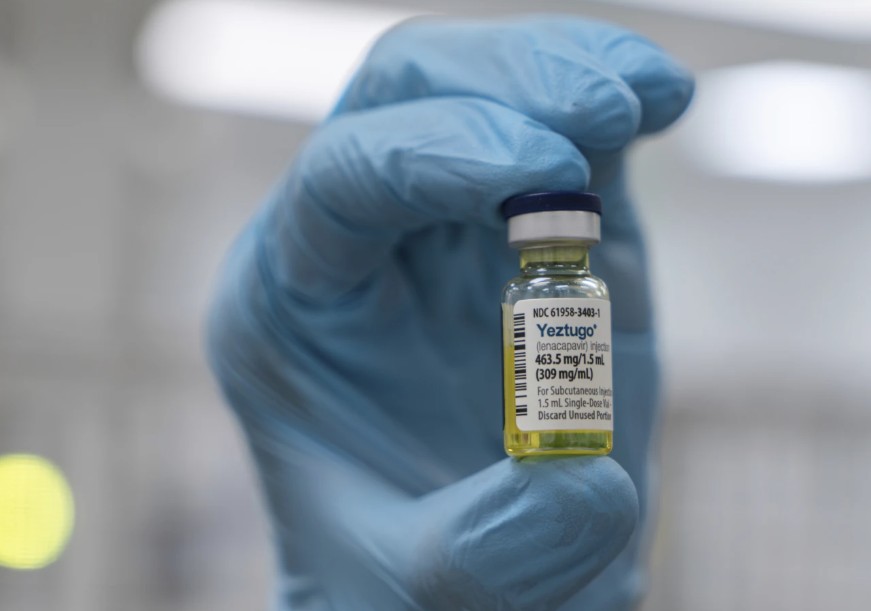
The World Health Organisation (WHO) has endorsed injectable lenacapavir (Leparavine) as a new option for HIV prevention, recommending its use twice a year.
The announcement was made at the 13th International AIDS Society Conference (IAS 2025), held in Kigali, Rwanda. This marks a significant step forward in HIV prevention efforts, particularly for communities that struggle with adherence to daily oral medications.
Lenacapavir is the first long-acting injectable HIV prevention drug that requires administration only twice a year. It offers a highly effective and convenient alternative to daily pills, making it especially valuable for individuals who face stigma, difficulties with daily adherence, or limited access to consistent healthcare.
Clinical trials have demonstrated lenacapavir’s remarkable effectiveness. Among more than 2,000 participants, only two cases of HIV were recorded. In trials involving women and adolescent girls in Africa—a population often underserved by current HIV prevention methods—lenacapavir provided complete protection.
WHO emphasised that despite the current limited availability of lenacapavir outside of clinical trials, countries should begin integrating it into national HIV prevention programs immediately. The organisation also called for careful monitoring of uptake, adherence, and overall impact during the rollout phase.
Dr Tedros Adhanom Ghebreyesus, WHO Director-General, described lenacapavir as the most promising advance in HIV prevention since antiretroviral therapy began, saying, “While an HIV vaccine remains out of reach, lenacapavir is the next best thing. With near-total protection shown in clinical trials, this injectable could be a game-changer for millions.”
To help remove one of the major barriers to HIV prevention, WHO is also promoting a simplified HIV testing approach based on rapid diagnostic tests. This strategy eliminates the need for complex laboratory infrastructure, allowing long-acting PrEP options like lenacapavir and cabotegravir to be delivered through more accessible, community-based platforms, including pharmacies, health clinics, and telehealth services.
WHO’s new guidance does not stop at prevention. The organisation has also released updated recommendations for HIV treatment and service delivery. Among these is the support for the use of long-acting injectable cabotegravir and rilpivirine for individuals who are stable on daily oral antiretroviral therapy.
WHO further encourages the integration of HIV care with services for noncommunicable diseases such as hypertension, diabetes, and mental health, recognising the importance of holistic and person-centred healthcare.
For individuals living with HIV who contract mpox, WHO now recommends the rapid initiation of antiretroviral therapy and HIV testing for anyone with suspected or confirmed mpox infection. The updated guidance also includes expanded screening for asymptomatic sexually transmitted infections, particularly within high-risk populations.
Recognising the increasing financial strain on health systems, WHO has also issued operational guidance to help countries safeguard essential HIV services. This includes frameworks for assessing risks, prioritising services, and adapting systems to maintain progress and protect health outcomes even in the face of shrinking budgets.
Dr Meg Doherty, Director of WHO’s Global HIV, Hepatitis and STI Programmes, highlighted the urgency of turning these recommendations into action. “We have the tools and the knowledge to end AIDS as a public health problem,” she said. “What’s needed now is bold action—grounded in equity and powered by communities.”
By the end of 2024, an estimated 40.8 million people were living with HIV globally, with 65 per cent of them residing in the African region. Around 630,000 people died from HIV-related causes during that year, while 1.3 million became newly infected, including 120,000 children. Access to treatment continues to expand, with 31.6 million people receiving antiretroviral therapy in 2024, up from 30.3 million the previous year.
Despite its promise, lenacapavir remains out of reach for most people in low-income countries due to its high cost.
Leparavine is currently priced at levels similar to those in developed countries, making it largely unaffordable for most Kenyans. While in the United States, Europe, and Canada, the cost ranges between $28,000 and $43,000 per year—equivalent to roughly 4 to 6.5 million Kenyan shillings—the price in Kenya is expected to be similar if no special subsidies or generic options become available.